A facelift, technically known as a rhytidectomy (from the Ancient Greek ῥυτίς (rhytis) ‘wrinkle’, and ἐκτομή (ektome) ‘excision’, the surgical removal of wrinkles), is a type of cosmetic surgery procedure intended to give a more youthful facial appearance. There are multiple surgical techniques and exercise routines. Surgery usually involves the removal of excess facial skin, with or without the tightening of underlying tissues, and the redraping of the skin on the patient‘s face and neck. Exercise routines tone underlying facial muscles without surgery. Surgical facelifts are effectively combined with eyelid surgery (blepharoplasty) and other facial procedures and are typically performed under general anesthesia or deep twilight sleep.
According to the most recent American Society for Aesthetic Plastic Surgery facelifts were the third most popular aesthetic surgery in 2019, surpassed only by rhinoplasty and blepharoplasty.[1]
Considering a facelift in turkey? This option has gained popularity due to its affordability and quality of care.
Pittsburg Press, 1 July 1906. p. 38.
Cutaneous period (1900–1970)
In the first 70 years of the 20th century, facelifts were performed by pulling on the skin on the face and cutting the loose parts off. The first facelift was reportedly performed by Eugen Holländer in 1901 in Berlin.[2] An elderly Polish female aristocrat asked him to: “lift her cheeks and corners of the mouth”. After much debate, he finally proceeded to excise an elliptical piece of skin around the ears. The first textbook about facial cosmetic surgery (1907) was written by Charles Miller (Chicago) entitled The Correction of Featural Imperfections.[3]
In the First World War (1914–1918), the Dutch surgeon Johannes Esser made one of the most famous discoveries in the field of plastic surgery to date, namely the “skin graft inlay technique,”[4] the technique was soon used on both English and German sides in the war. At the same time, the British plastic surgeon Harold Delfs Gillies used the Esser-graft to school all those who flocked towards him who wanted to study under him. That’s how he earned the name “Father of 20th Century Plastic Surgery”. In 1919, Dr Passot was known to publish one of the first papers on face-lifting, this consisted mainly of the elevating and redraping of the facial skin. After this, many others began to write papers on face-lifting in the 1920s. From then, the esthetic surgery was being performed on a large scale, form the basis of the reconstructive surgery. The first female plastic surgeon, Suzanne Noël, played a large role in its development and she wrote one of the first books about esthetic surgery named Chirurgie Esthetique, son rôle social.
Why Choose a Facelift in Turkey?
Expert Insights on Facelift in Turkey
Dr. Gorkem Atsal: At our clinic in Istanbul, we offer several types of facelift procedures, including the mini facelift, SMAS facelift, and neck lift — each designed to meet the unique needs of our patients. However, my preferred technique is the deep plane facelift, as it allows for a more comprehensive and natural-looking rejuvenation. By lifting the deeper facial layers rather than just the skin, we can achieve more dramatic and longer-lasting results, especially in the midface, jowls, and neck area. Many patients from around the world travel for facelift surgery in Turkey because of the combination of medical expertise, advanced techniques, and personalized care. For those seeking to truly restore youthful facial contours without an artificial or pulled look, the deep plane facelift remains the gold standard — and it’s the technique I trust most to deliver the transformative yet natural outcomes my patients deserve.
SMAS period (1970–1980)
In 1968, Tord Skoog introduced the concept of subfacial dissection, therefore providing suspension of the stronger deeper layer rather than relying on skin tension to achieve his facelift (he publishes his technique in 1974, with subfacial dissection of the platysma without detaching the skin in a posterior direction).[5] In 1976, Mitz and Peyronie described the anatomical Superficial Musculoaponeurotic System, or SMAS,[6] a term coined by Paul Tessier, Mitz and Peyronie’s tutor in craniofacial surgery, after he had become familiar with Skoog’s technique. After Skoog died of a heart attack, the superficial muscular aponeurotic system (SMAS) concept rapidly emerged to become the standard face-lifting technique, which was the first innovative change in facelift surgery in over 50 years.[7]
Deep plane period (1980–1991)
Tessier, who had his background in the craniofacial surgery, made the step to a subperiosteal dissection via a coronal incision.[8] In 1979, Tessier demonstrated that the subperiosteal undermining of the superior and lateral orbital rims allowed the elevation of the soft tissue and eyebrows with better results than the classic face-lifting. The objective was to elevate the soft tissue over the underlying skeleton to re-establish the patient’s youthful appearance.
Volumetric period (since 1991)
At the start of this period in the history of the facelift, there was a change in conceptual thinking, surgeons started to care more about minimizing scars, restoring the subcutaneous volume that was lost during the ageing process and they started making use of a cranial direction of the “lift” instead of posterior.
The technique for performing a facelift went from simply pulling on the skin and sewing it back to aggressive SMAS and deep plane surgeries to a more refined facelift where variable options are considered to have an aesthetically good and a more long-lasting effect.
Indications
A facelift is performed to rejuvenate the appearance of the face. Aging of the face is most shown by a change in position of the deep anatomical structures, notably the platysma muscle, cheek fat and the orbicularis oculi muscle.[9] These lead up to three landmarks namely, an appearance of the jowl (a broken jaw line by ptosis of the platysma muscle), increased redundancy of the nasolabial fold (caused by a descent of cheek fat) and the increased distance from the ciliary margin to the inferior-most point of the orbicularis oculi muscle (caused by decreasing tone of the orbicularis oculi muscle).[9] The skin is a fourth component in the aging of the face. The ideal age for face-lifting is at age 50 or younger, as measured by patient satisfaction.[10]
Contraindications
Contraindications to facelift surgery include severe concomitant medical problems, both physical and psychological. While not absolute contraindications, the risk of postoperative complications is increased in cigarette smokers and patients with hypertension and diabetes.[11] Patients are typically asked to abstain from taking aspirin or other blood thinners for at least one week prior to surgery. Patients motivations and expectations are an important factor in order to determine the patient’s medical status. A psychiatric illness leading to unreasonable expectations for the surgical outcome, such as a distorted perception of reality, can be a contraindication to surgery.
Surgical anatomy
A dissection in the deep plane can mostly be performed safely, because the facial nerve innervates the facial muscles on the deep surface of these muscles (except for the muscles which are lying deep to the facial nerve, the mentalis, the levator anguli oris and the buccinator). The fibres of the nerve are becoming more superficially medially. Therefore, the dissection of a deep plane begins further away of the surface then it ends. This allows the undermining to be carried out towards the nasolabial fold without harming the branches of the facial nerve.
Retaining ligaments
The retaining ligaments in the face provide an anchorage of superficial structures to underlying bone. Four retaining ligaments exist.[12] The platysma-cutaneous ligaments and the platysma-auricular ligament are aponeurotic condensations which connect the platysma to the dermis. The osteocutaneous ligaments, the zygomatic ligament and the mandibular ligament, are more important. They attach to the skin and bone, leading to a counteraction of gravitational forces. These ligaments should be released surgically to obtain a fully mobile facelift flap.
- Nasolabial folds
- Melolabial folds (marionette lines)
- Greater auricular nerve
Injury to the greater auricular nerve is the most seen nerve injury after rhytidectomy.[13,14] Care should be taken in elevation over the sternocleidomastoid muscle, because of the terminal branches of the nerve that pass superficially to innervate the earlobe.
Procedures
Many different procedures are used for rhytidectomy.[15] The differences are mostly the type of incision, the invasiveness and the area of the face that is treated. Each surgeon practices multiple different types of facelift surgery. At a consultation the procedure with the best outcome is chosen for every patient. Expectations of the patient, the age, possible recovery time and areas to improve are some of the many factors taken in consideration before choosing a technique of rhytidectomy.
In the traditional facelift, an incision is made in front of the ear extending up into the hairline. The incision curves around the bottom of the ear and then behind it, usually ending near the hairline on the back of the neck. After the skin incision is made, the skin is separated from the deeper tissues with a scalpel or scissors (also called undermining) over the cheeks and neck. At this point, the deeper tissues (SMAS, the fascial suspension system of the face) can be tightened with sutures, with or without removing some of the excess deeper tissues. The skin is then redraped, and the amount of excess skin to be removed is determined by the surgeon’s judgement and experience. The excess skin is then removed, and the skin incisions are closed with sutures and staples.
SMAS lift
The SMAS (Superficial Musculo Aponeurotic System) layer consists of suspensory ligaments that encase the cheek fat, thereby causing them to remain in their normal position. This procedure is often performed in tandem with blepharoplasty as an ancillary procedure.[16,17] Resuspension and securing the SMAS anatomical layer can lead to rejuvenation of the face, by counteracting aging and gravity caused laxity.[17] Modifications to this technique led to development of the “Composite Facelift” and “Deep plane Facelift.”[18]
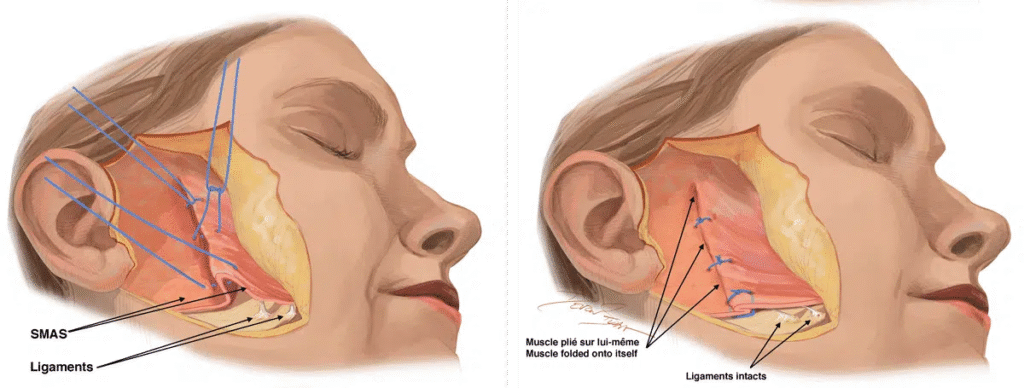
The surgery is taking place under the skin. The muscle is not released. Rather sutures are placed to fold it onto itself. Because the muscle is not released from the deeper layers, this technique may cause stretching and tension and the result may not be as long lasting.
Deep-plane facelift
In order to correct the deepening of the nasolabial fold more accurately, the deep plane facelift was developed. Differing from the SMAS lift by freeing cheek fat and some muscles from their bone implement. This technique is superior and sophisticated than SMAS lift. The SMAS lift can be an effective procedure to reposition the platysma muscle; however, the nasolabial fold better addressed by a deep plane facelift or composite facelift.
At our clinic in Istanbul, we perform the deep plane facelift as one of the most advanced facial rejuvenation procedures available today. Unlike traditional techniques that only lift the skin, the deep plane method repositions the underlying muscle and fat layers for a more natural and long-lasting result. This technique is especially effective for addressing deep nasolabial folds, sagging cheeks, and jawline laxity. Many international patients choose to have their facelift surgery in Turkey not only for the high medical standards but also for the personalized care and affordability. As a surgeon deeply committed to aesthetic harmony, I always tailor each procedure to the patient’s facial anatomy, ensuring results that enhance rather than alter their natural beauty. When done correctly, a deep plane facelift can take years off one’s appearance without looking tight or overdone — and that’s exactly what we aim for here at our clinic.
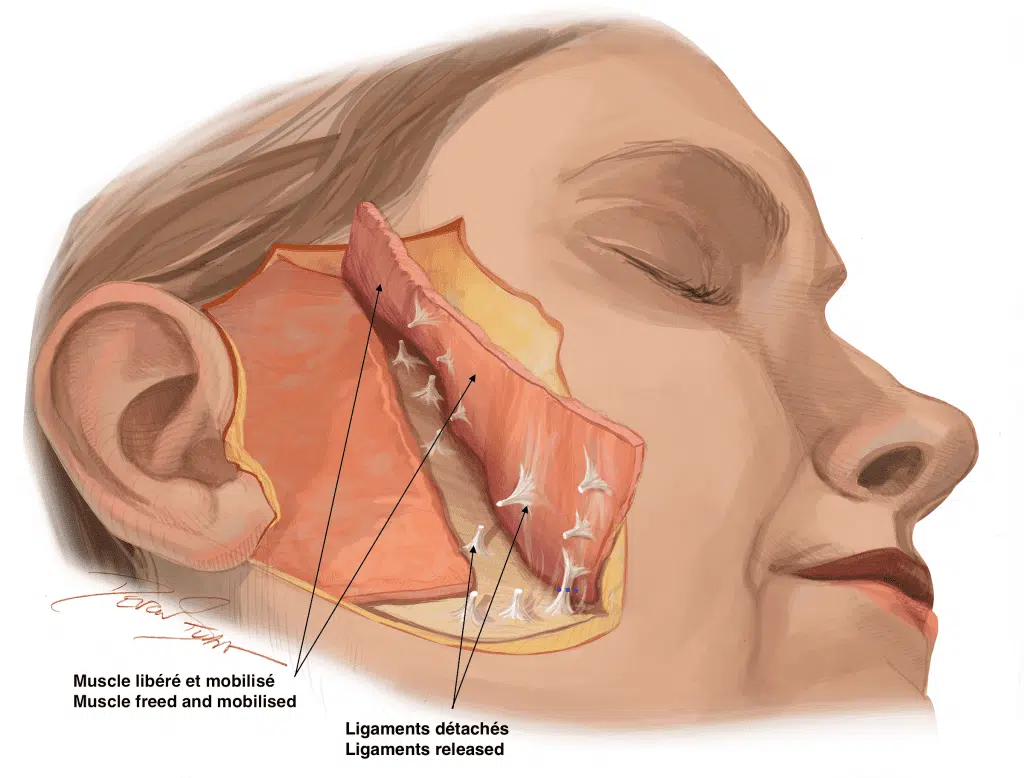
Deep plane facelift. The surgery takes place under the muscle. The ligaments are released.
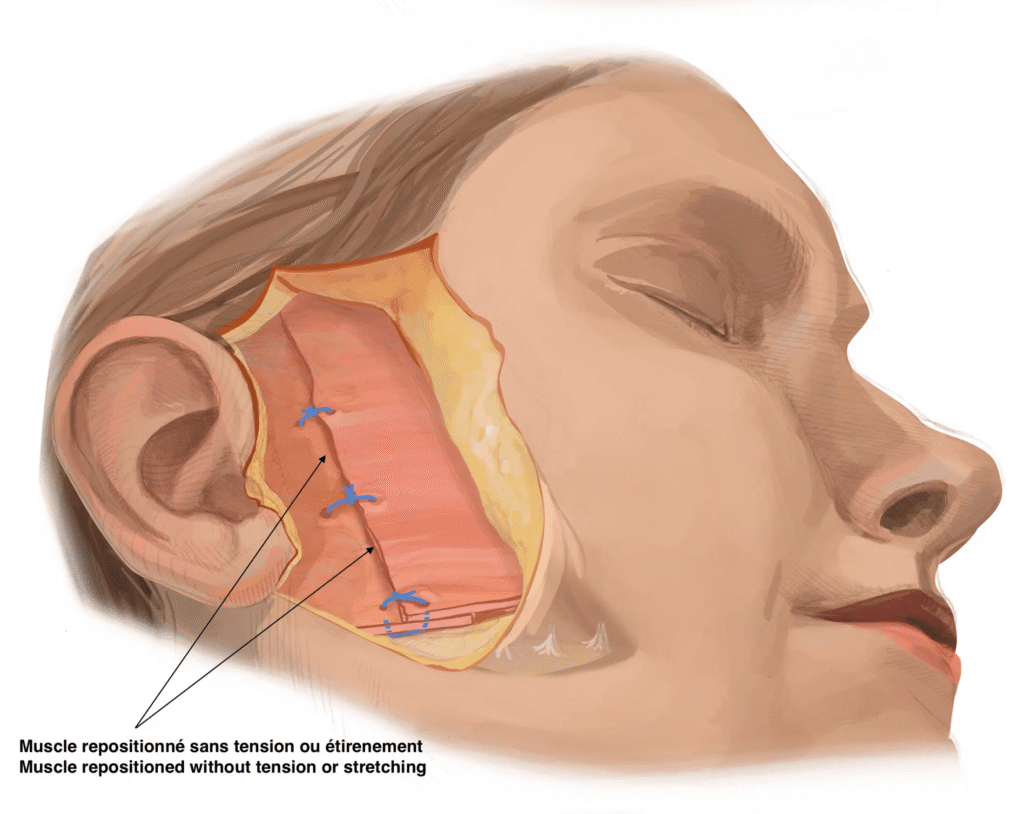
The muscle is then lifted and repositioned more freely and without tension or stretch.
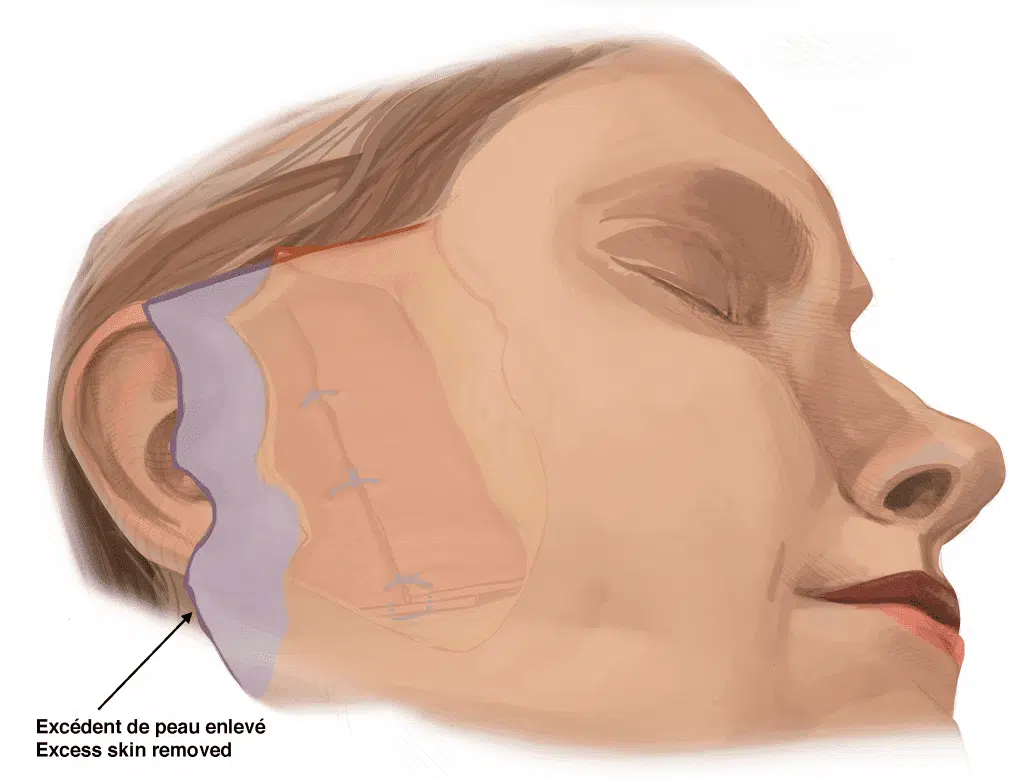
The excess skin is then removed.
Composite facelift
As well as in the deep plane facelift, in the composite facelift a deeper layer of tissue is mobilised and repositioned. The difference between these operating techniques is the extra repositioning and fixation of the orbicularis oculi muscle in the composite facelift procedure. The malar crescent caused by the orbicularis oculi ptosis can be addressed in a composite facelift.
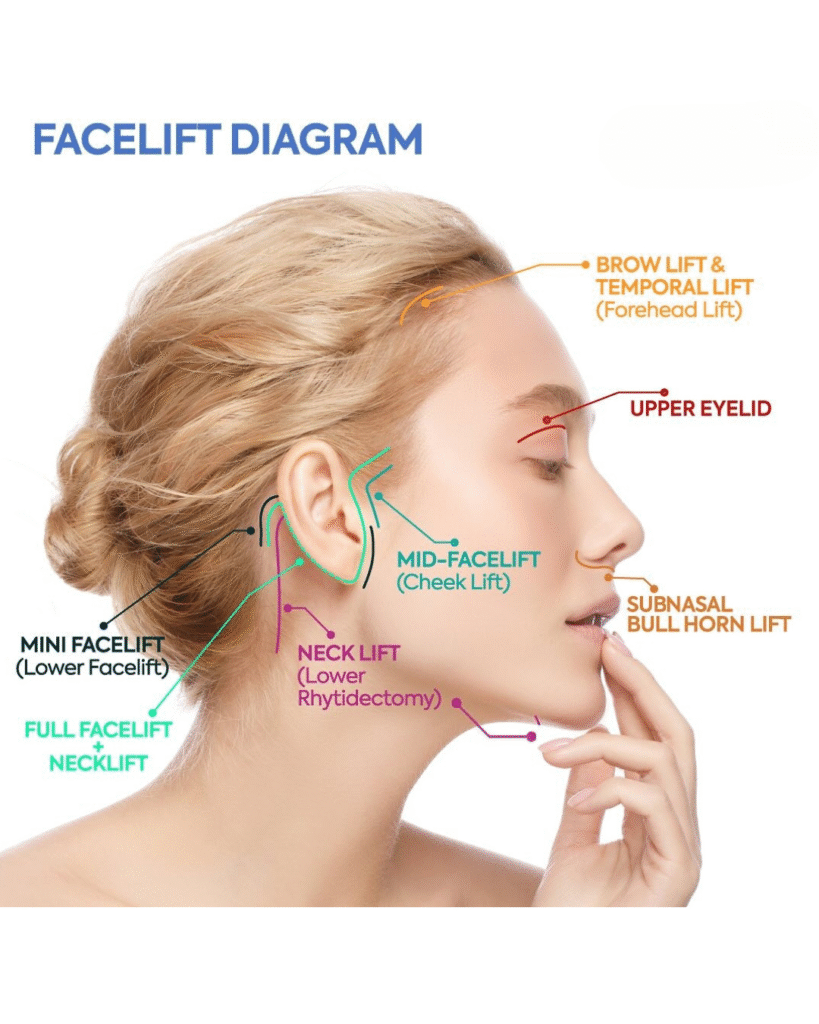
Mid face-lift
The mid face area, the area between the cheeks, flattens and makes a woman’s face look slightly more masculine. The mid face-lift is suggested to people where these changes occur, yet without a significant degree of jowling or sagging of the neck. In these cases a mid face-lift is sufficient to rejuvenate the face opposed to a full facelift, which is a more drastic surgery. The ideal candidates for a mid face-lift is when a person is in his or her 40s, or if the cheeks appear to be sagging and the nasolabial area has laxity or skin folds. To achieve a younger appearance the surgeon makes several small incisions along the hairline and inside the mouth, this way the fatty tissue layers can be lifted and repositioned. This way there are practically no scars. The fatty layer that lies over the cheekbones is also lifted and repositioned. This improves the nose-to-mouth lines and the roundness over the cheekbones. The recovery time is rather short and this procedure is often combined with a blepharoplasty (eyelid surgery).
Mini-facelift
The mini-facelift is the least invasive type of facelift. It is also called the ‘S’ lift because of the shape of the incision that is used or the ‘short-scar’ facelift. This lift is a more temporary solution to the ageing of the face which also has less downtime and is done on people who have deep nasolabial folds, sagging facial structures, yet still have a firm and well-contoured neck.[19]
Subperiosteal facelift
The subperiosteal facelift technique is done by vertically lifting the soft tissues of the face, completely separating it from the underlying facial bones and elevating it to a more esthetically pleasing position, correcting deep nasolabial folds and sagging cheeks. The difference between this and other lifts is that the subperiosteal facelift has a longer period of facial swelling after the procedure.
Skin-only facelift
With the skin-only facelift only the skin of the face is lifted and not the underlying SMAS, muscles or other structures. It can be done with a simple ellipse of skin removed with minimal undermining of skin flaps or more extensively with large skin flaps. It can last a couple of years but some patients may want a touch-up at 6 to 12 months after the procedure. The reason that this option is considered is that it has fewer complications and quicker recovery.
Thread lift
A temporary technique called thread lift or non-surgical face lift simplifies the operation. Silicone or dissolvable threads with barbs are used to pull the face and neck skin upwards without the need of skin excision.
MACS facelift
The term MACS-lift – or Minimal Access Cranial Suspension lift – allows for the correction of sagging facial features through a short, minimal incision, elevating them vertically by suspending them from above. The main disadvantage is short-lasting results about 2-3 months.
Complications
The most common complication is bleeding which usually requires a return to the operating room. Less common complications may include damage to the facial nerves and necrosis of the skin flaps or infection. Although the facial plastic surgeon attempts to prevent and minimise the risk of complications, a rhytidectomy may have complications.
Hematoma is the most seen complication after rhytidectomy. Almost all of the hematomas occur within the first 24 hours after the rhytidectomy.[13,14,20]
Nerve injury can be sustained during rhytidectomy. This kind of injury can be temporary or permanent and harm can be done to either sensory or motor nerves of the face. As a sensory nerve, the great auricular nerve is the most common nerve to get injured at a facelift procedure.[14,20] The most injured motor nerve is the facial nerve.[14,21]
Skin necrosis can occur after a facelift operation. Smoking increases the risk of skin necrosis 12-fold.[11] Scarring is considered a complication of facelift surgery. Hypertrophic scars can appear. A facelift requires skin incisions; however, the incisions in front of and behind the ear are usually inconspicuous.
Hair loss in the portions of the incision within the hair-bearing scalp can rarely occur. A distortion of the hairline—and facial hair in men—can result after a rhytidectomy. In men, the sideburns can be slightly pulled backwards and upwards. Achieving a natural appearance following surgery in men can be more challenging due to their hair-bearing preauricular skin. In both men and women, one of the signs of having had a unproffesional facelift can be an earlobe which is pulled forwards and/or distorted. If too much skin is removed, or a more vertical vector not employed, the face can assume a pulled-back, “windswept” appearance.
One of the most often overlooked (or not discussed) areas of a traditional facelift procedure is the effects on the anatomical positioning and angles of the ears, especially under inexperienced hands
Infection is a rare complication for patients who have undergone a rhytidectomy.[22] Staphylococcus is the most usual causative organism for an infection after facelift surgery.[13]
References
1.”Plastic Surgery Statistics”. American Society of Plastic Surgeons. Retrieved 19 October 2022.
2.Panfilov, Dimitrije E. (2005). Cosmetic Surgery Today. Trans. Grahame Larkin. New York, N.Y.: Thiene. p. 4. ISBN 978-1-58890-334-1.
3.Kita, Natalie. “The History of Plastic Surgery”. Archived from the original on 19 November 2012. Retrieved 10 March 2009.
4.van Bergen, Leo. “Mens of monster? Plastische chirurgie en de Eerste Wereldoorlog”.
5.Skoog, Tord Gustav (1974). Plastic Surgery: New Methods and Refinements. Saunders. p. 500. ISBN 978-0721683553.
6.Mitz, V.; Peyronie M. (July 1976). “The superficial musculo-aponeurotic system (SMAS) in the parotid and cheek area”. Plast Reconstr Surg. 1. 58 (1): 80–8. doi:10.1097/00006534-197607000-00013. PMID 935283. S2CID 19719594.
7.Tessier, P. (September 1979). “Facelifting and frontal rhytidectomy”. Transactions of 7th International Conference on Plastic and Reconstructive Surgery.
8.Heinrichs, HL; Kaidi, AA (September 1998). “Subperiosteal face lift: a 200-case, 4-year review”. Plastic and Reconstructive Surgery. 102 (3): 843–55. doi:10.1097/00006534-199809030-00036. PMID 9727455.
9.Hamra, S.T. (April 1997). “Composite Rhytidectomy”. Plast Reconstr Surg. 24 (2): 1–13.
10.Marcus, BC (August 2012). “Rhytidectomy: current concepts, controversies and the state of the art”. Current Opinion in Otolaryngology & Head and Neck Surgery. 20 (4): 262–6. doi:10.1097/MOO.0b013e328355b175. PMID 22894994. S2CID 39343579.
11.Rees, TD; Liverett, DM; Guy, CL (June 1984). “The effect of cigarette smoking on skin-flap survival in the face lift patient”. Plastic and Reconstructive Surgery. 73 (6): 911-5. doi:10.1097/00006534-198406000-00009. PMID 6728942.
12.Furnas, DW (January 1989). “The retaining ligaments of the cheek”. Plastic and Reconstructive Surgery. 83 (1): 11–6. doi:10.1097/00006534-198901000-00003. PMID 2909050. S2CID 1098358.
13.Moyer, JS; Baker, SR (August 2005). “Complications of rhytidectomy”. Facial Plastic Surgery Clinics of North America. 13 (3): 469–78. doi:10.1016/j.fsc.2005.04.005. PMID 16085292. S2CID 28878512.
14.Baker, DC (July 1983). “Complications of cervicofacial rhytidectomy”. Clinics in Plastic Surgery. 10 (3): 543–62. doi:10.1016/S0094-1298(20)31873-3. PMID 6627843.
15.”Facelift (rhytidectomy) approach”.
16.Vallecillos, Dr Glenn (4 August 2022). “Deep Plane Facelift Versus SMAS Facelift Demystified Glenn Vallecillos, MD, FACS”. Retrieved 28 October 2022.
17.Joshi, Kritika; Hohman, Marc H.; Seiger, Eric (2022), “SMAS Plication Facelift”, StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 30285353, retrieved 28 October 2022
18.”Composite Facelift: Background, History of the Procedure, Problem”. medscape.com. 22 November 2021.
19.”Endoscopic Facelift”. Al Shunnar Plastic Surgery. Retrieved 14 June 2022.
20.Rees, TD; Aston, SJ (January 1978). “Complications of rhytidectomy”. Clinics in Plastic Surgery. 5 (1): 109–19. doi:10.1016/S0094-1298(20)32193-3. PMID 639438.
21.Baker, DC; Conley, J (December 1979). “Avoiding facial nerve injuries in rhytidectomy. Anatomical variations and pitfalls”. Plastic and Reconstructive Surgery. 64 (6): 781–95. doi:10.1097/00006534-197912000-00005. PMID 515227. S2CID 23475490.
22.LeRoy JL, Rees TD, Nolan WB (March 1994). “Infections requiring hospital readmission following face lift surgery: incidence, treatment, and sequelae”. Plastic and Reconstructive Surgery. 93 (3): 533–6. doi:10.1097/00006534-199493030-00013. PMID 8115508.